Hello dear blog and blog readers,
I am sorry I've been so absent from you. What with this ongoing Costochondritis that feels like nails being pounded into my ribs, well, it's been fun. And ongoing. And not really fun. And ongoing.
I've also been looking after a wild european hedgehog that has chronic lung disease. He's almost died a couple times but finally seems to be pulling through, fingers crossed. I hope to be blogging more, but I'm also attempting my homeschool exemption for Miss S, so, time is limited.
Instead of updating you on life with TRAPS, which is doing the sort-of-not-fun-mostly-sucky thing, I'll answer some of your most burning questions.
And, because most of it is miscarriage related, welcome to those of you who have loved and lost and welcome to those of you just wanting to know more about miscarriage.
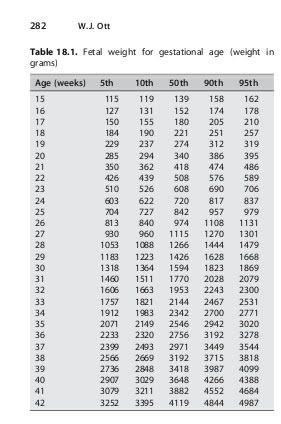
1) What is the average fetal weight?Good Question!
I hope this jpg answers your questions. Those weights are in grams, so you'll have to convert to ounces, then to pounds.
 2) What is the prevalence for twins?
2) What is the prevalence for twins?
The prevalence of twin gestation varies from 1% to 5% depending on gestational age at assessment, as a significant number of twins suffer intrauterine fetal demise of one of the pair [2]. The overall incidence of spontaneous twin gestations has declined, but reproductive technologies, including ovulation induction and surgical transfer of gametes or ova, have resulted in an increasing number of high-order multiple gestations [2]. Doppler Ultrasound in Obstetrics and Gynecology, edited by Dev Maulik.
You can get a copy of that book here:
link3) Process of ConceptionI covered conception in the last Jen Answers Your Questions, but I'll go through it again.
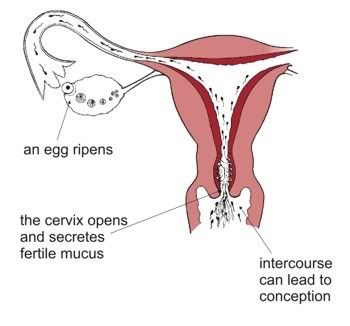
Firstly, the brain secretes hormones to tell one of the ovaries to begin maturing some follicles. The follicles race to see who will get to about 20mm in size first. As the follicles begin to reach the size needed for healthy ovulation, the brain begins to reverse the hormones, and instead, forcing the luetenizing hormone really high. This is called the Lh surge.
A single egg, or ova, pops forth from the ovary, causing the others to immediately seize in their race to maturation and they die off. It's a myth that only one egg matures each cycle. Only 1 mature egg pops forth, but there can be up to 5 follicles that were maturing eggs. Hence why you lose eggs faster than just 1 a month for the duration of your life.
There are plenty of occasions when the Lh surge can trigger another follicle to rupture, but the ova inside may not be a healthy egg and may not conceive. However, it might and that's generally how you get fraternal twins.
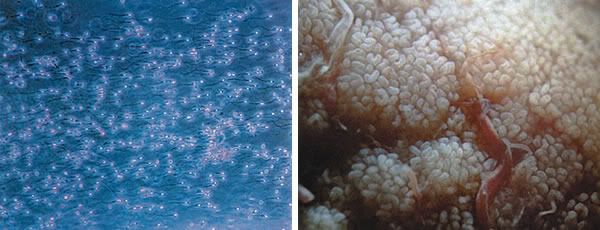
The egg is then swept up by the tiny little hair like fronds of the fallopian tubes. Think of the fallopian tube like one of those awesome anemones Nemo lived in. Just like that.
The egg is swept down past the little hairs who tidy it up and about half-way down, the egg meets sperm. It is essential the sperm is waiting for the egg otherwise they just miss each other like ships passing in the night.
This is where Conception happens!

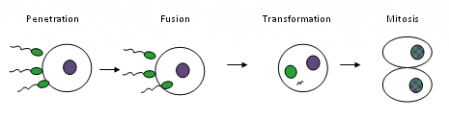
The sperm, attracted by a jelly like substance that protects the egg, race towards it, pushing head first into the jelly. The jelly, reacting with the sperm, creates an acidic liquid that bores past the hard outer shell of the egg. Only 1 sperm can make a healthy baby, but sadly, often more than 1 can get into the egg. The result is a miscarriage.
So, once the sperm has hit into the orb of the ova, the acids in the ova begin to destroy the sperm, pulling it apart as the sperm now becomes a physical entity within the ova and the dna begins to rapidly mingle with that of the ova.
Various bits of the sperm are used to create the new single cell of life. Nothing is wasted here.
Some argue that the ova actually chooses which sperm will bore past the jelly by attracting certain sperm with pheromones. Pretty cool, actually.
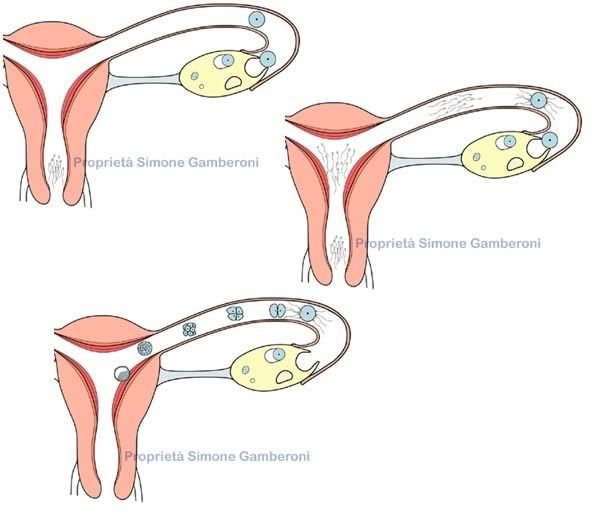
From there, the rapidly developing and growing blastocyst falls from the tube into the uterus where it must fall into a groove like area and begin dissolving the tissue.
If successful, the blastocyst will become an embryo. If not, the pregnancy fails.
This is one of the most error filled parts of the journey. Too much dissolving will force the body to reject it. Not enough and it will be discarded.
This ultra-important stage is called Implantation.
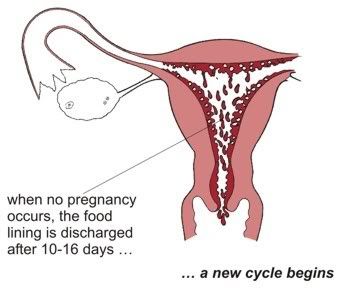
And, finally, if the whole process was unsuccessful, the body begins to bleed, cycle again.
 4) Yetis with steroids
4) Yetis with steroids 5) Why do People Miscarry?
5) Why do People Miscarry?Gosh. I wish I knew why. Logically, my head tells me because it's because of things like corrupted dna or sperms with bad tails. Mixed RNA that doesn't become a baby. Or a baby who doesn't implant or a uterus who opens too soon.
Emotionally, I wish it never happened. But it does.
Does it happen to teach us something? No. There is no *point* in miscarriage. If you do learn something, well, consider that wisdom. But there is no rhyme or reason why a body miscarries.
It just does.
Check out
Unspoken Grief.
6) Why do i see a black spot at 5 week ultrasound?What you are seeing is the post-blastocyst stage of pregnancy which isn't yet the classic space alien or shrimp dude who wiggles.
We call this the Gestational Sac.

"The gestational sac is often the first thing that most transvaginal ultrasounds can detect at about 5 weeks. This is seen before a recognizable embryo can be seen. Within this week, at about week 5 ½ to the beginning of the 6th week, a yolk sac can be seen inside the gestational sac. The yolk sac will be the earliest source of nutrients for the developing fetus."
source
"The gestational sac (or gestation sac) is the only available intrauterine structure that can be used to determine if an intrauterine pregnancy (IUP) exists, until the embryo is identified.
On ultrasound, it is an anechoic (dark) space surrounded by a hyperchoic (white) rim.
It is spherical in shape, and usually located in the upper uterine fundus.
The mean sac diameter (MSD) is an effective estimate of gestational age[1] between 5 and 6 weeks, with an accuracy of about +/- 5 days. [2]
The yolk sac and embryo should be readily identified when the gestational sac reaches a certain size -- a yolk sac should be seen when gestational sac is 20mm and a fetal pole should be seen when the gestational sac reaches 25mm."
source 7) When do you see a fetal pole in a sonogram?
7) When do you see a fetal pole in a sonogram? "Fetal pole, a thick spot near the yolk sac, is the term used for the earliest signs of a baby in an early pregnancy ultrasound -- before the baby has formed a recognizable human shape. With a transvaginal ultrasound, the fetal pole becomes visible around 6 weeks of gestation."
source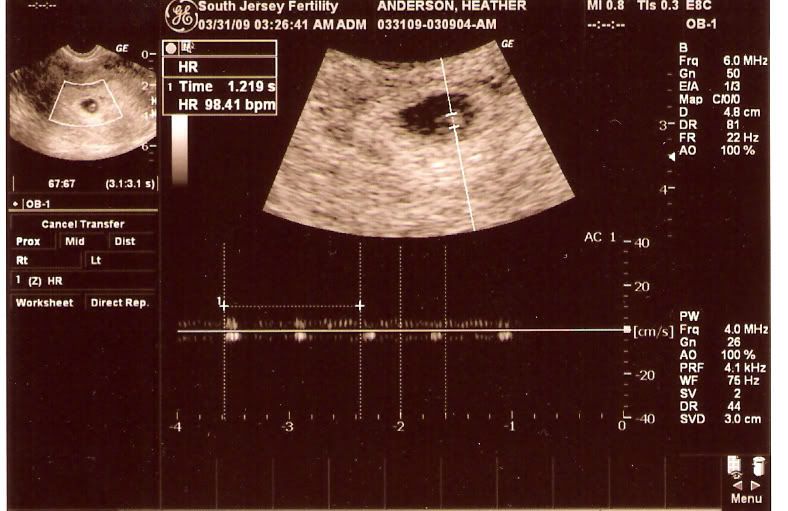
Ultrasound used
without permission.
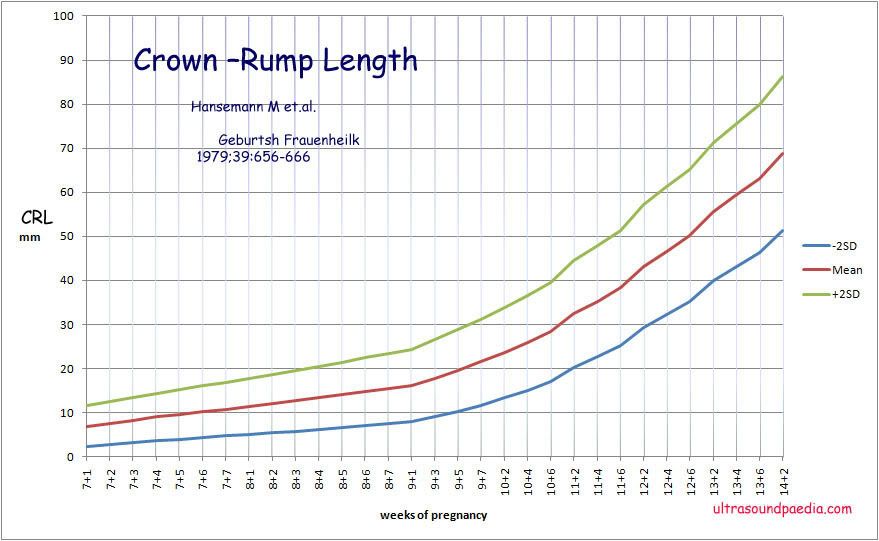
"The fetal pole is a thickening on the margin of the yolk sac of a fetus during pregnancy. It is usually identified at 6.5 weeks with abdominal ultrasound imaging, and 6 weeks with vaginal ultrasound imaging. However it is quite normal for the fetal pole to not be visible until about 9 weeks. The fetal pole may be seen at 2–4 mm crown-rump length (CRL), and heart motion is often detected when it is seen. In the embryo, the heartbeat is seen as a regular flutter, which should be first evident at 5 mm CRL. If the embryo is less than 5 mm CRL, it is possible for it to be healthy without showing a heartbeat, though a follow up study in 5–7 days will almost always demonstrate the heartbeat."
source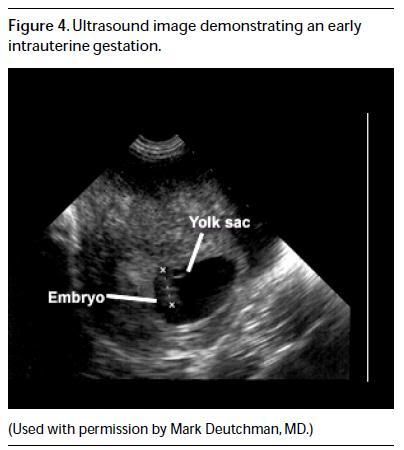
Ultrasound used
without permission, not as stated.
"5 ½ to 6 ½ weeks is usually a very good time to detect either a fetal pole or even a fetal heart beat by vaginal ultrasound. The fetal pole is the first visible sign of a developing embryo. This pole structure actually has some curve to it with the embryo’s head at one end and what looks like a tail at the other end. The fetal pole now allows for crown to rump measurements (CRL) to be taken, so that pregnancy dating can be a bit more accurate. The fetal pole may be seen at a crown-rump length (CRL) of 2-4mm, and the heartbeat may be seen as a regular flutter when the CRL has reached 5mm.
If a vaginal ultrasound is done and no fetal pole or cardiac activity is seen, another ultrasound scan should be done in 3-7 days. Due to the fact that pregnancy dating can be wrong, it would be much too early at this point to make a clear diagnosis on the outcome of the pregnancy."
source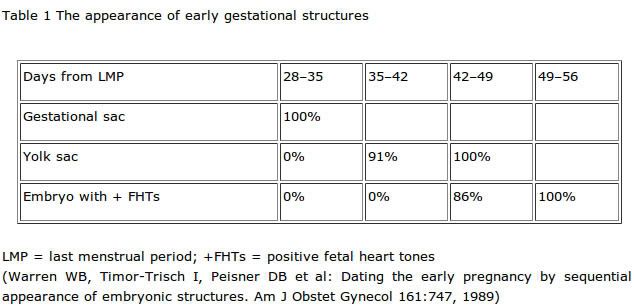
 8) What week do miscarriages usually occur?
8) What week do miscarriages usually occur? Miscarriage is a common event of
early pregnancy. It is less common in the 2nd Trimester and even less common in the 3rd Trimester, when it is considered stillbirth or antenatal/neonatal death.
So, from the time of conception until the end of the first trimester is the time when most miscarriages occur. I know that's not helpful but it's the logical answer. I have known women who miscarry early in the first trimester and some who miscarry just before the 2nd trimester. To me, there is no first trimester 'time' that is riskier than any other first trimester 'time'.
However, some people have noted
more miscarriages between certain weeks.
Ask Dr. Sears -- "Most miscarriages occur before the eighth week of pregnancy. As your pregnancy progresses, the chance of miscarriage decreases."
sourceAmerican Pregnancy -- "Most miscarriages occur during the first 13 weeks of pregnancy."
sourceMedicineNet -- "Miscarriage occurs in about 15% to 20% of all recognized pregnancies, and usually occurs before the 13th week of pregnancy.">
sourceAbout.com -- "As pregnancy progresses, miscarriage risk decreases. Most estimates state that 80% of miscarriages happen before 12 weeks of pregnancy.
Because 80% of miscarriages happen in the first trimester, the overall risk of miscarriage after the first trimester is about 3%.">
sourceBabyCenter -- " About 10 to 20 percent of known pregnancies end in miscarriage, and more than 80 percent of these losses happen before 12 weeks."
source9) What does tissue look like during a miscarriage?I can only answer for myself here, but there is a clear definition between uterine lining, which is dark red, bloody and more meat like. The fetal tissue is often a purple sort of colour or even a light grey. It is more like a cooked chicken thigh in texture.
10) What does pleurisy look like in a xray?
Credit: ZEPHYR/SCIENCE PHOTO LIBRARY
Caption: Pleurisy. Coloured X-ray of the lungs of a patient with pleurisy, inflammation of the membranes (pleura) that line the chest cavity and lungs. A large area of inflammation (white) is seen obstructing the lung at bottom right. Inflammation of the pleura leads to the lungs rubbing against the chest wall, which causes sharp pain on breathing. Fluid may accumulate in the space between the membranes, causing breathing difficulties. Treatment is of the underlying cause, which in this case is a Staphylococcus infection, but may be a viral infection, cancer or an embolism.

Credit: ZEPHYR/SCIENCE PHOTO LIBRARY
Caption: Pleurisy. Coloured X-rays of the lungs of a 65 year old patient with pleurisy, an inflammation of the membranes (pleura) that line the chest cavity and lungs. In the left image, a large area of inflammation is obstructing the patient's right lung (white mass at centre left). Inflammation of the pleura leads to the lungs rubbing against the chest wall, which causes sharp pain on breathing. In this case, fluid had accumulated in the space between the membranes, causing breathing difficulties, so the lung needed to be drained to remove it. The right image shows the lung after drainage of the fluid. The underlying cause will also need to be treated, which may be a bacterial infection, viral infection, cancer or an embolism.
11) What does an ultrasound look like after a miscarriage?The uterus should show no signs of inflammation, retained tissue or blood clots. The uterus should look as though it is at the pre-ovulatory stage post menses.
This is an empty, normal, non-pregnant uterus:
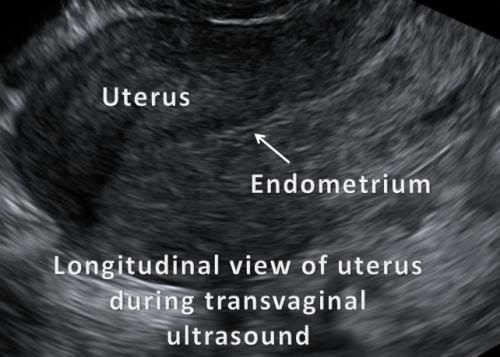
There is nothing here. No adhesions, no swelling, no clotting.
This is what a post-miscarriage womb should look like.
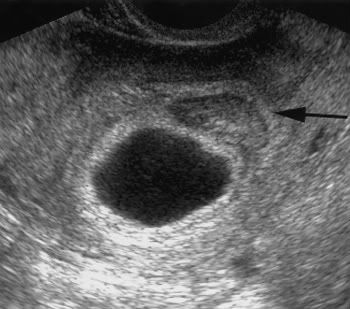
This is a womb with retained tissue:

Though it is small, you can clearly see there is retained tissue inside this womb.
As I have had dramatic issues with retained tissue, I want you to know the signs.
Symptoms of Incomplete Miscarriage"The main signs of incomplete miscarriage are bleeding and cramping. A woman with these symptoms should see a doctor to determine whether the bleeding and cramping are due to miscarriage or some other factor. If the doctor diagnoses a miscarriage, the woman may have a D & C or choose to wait for the miscarriage to complete naturally.
About 90% of the time, a miscarriage that is incomplete at the time of the initial miscarriage diagnosis will complete without intervention should the woman wish to avoid a D & C. Sometimes, however, tissue remains in the uterus without the body passing it naturally.
If bleeding and cramping continue for longer than two weeks, the woman may have retained tissue in the uterus that can pose a risk of infection if not treated."
source bolding is mine
Post D&C Retained Tissue -- "Retained tissue" means tissue that remains in the uterus after the surgery is over. Symptoms of retained tissue might be excessive bleeding, large blood clots and intense cramping.12) What does a partial molar pregnancy look like?Firstly, what is a partial molar pregnancy?
"In most partial molar pregnancies, the fertilized egg has the normal set of chromosomes from the mother and two sets from the father, so there are 69 chromosomes instead of the normal 46. (This can happen when chromosomes from the sperm are duplicated or when two sperm fertilize the same egg.)
In a partial molar pregnancy, there's some normal placental tissue among the cluster of abnormal tissue. The embryo does begin to develop, so there may be a fetus or just some fetal tissue or an amniotic sac. But even if a fetus is present, in most cases it's so abnormal that it can't survive."
source 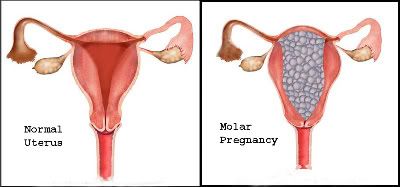
With my twin loss, because of the hemorrhaging I had, it was considered a suspected twin/partial molar, but none of the lab work showed that it was a molar pregnancy.
This image shows a twin/molar pregnancy as well as 2 moles and a partial molar pregnancy.
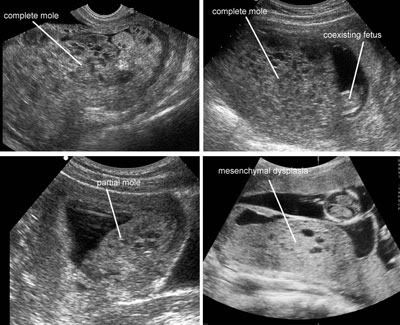
One of the unique features of a molar or partial molar pregnancy is that the genetically corrupted placental dna forms the tissue into small grape like cysts. You can pass these vaginally.

Now you can see why they make this strange looking ultrasound.
 13) You gain strength courage and confidence eleanor roosevelt
13) You gain strength courage and confidence eleanor roosevelt
You gain strength, courage and confidence by every experience in which you really stop to look fear in the face. You are able to say to yourself, 'I have lived through this horror. I can take the next thing that comes along.' You must do the thing you think you cannot do.
Eleanor Roosevelt
US diplomat & reformer (1884 - 1962)
14) Xray of an ectopic pregnancy This was a bit of an unusual request as I can't imagine *any* situation where someone would voluntarily xray a pregnancy woman.
If you meant an 'ultrasound of an ectopic pregnancy', well, that's different.
What is an ectopic pregnancy?

An ectopic pregnancy is one that occurs in an abnormal place(outside the uterus). Ectopic pregnancies can occur in many parts of the reproductive system, but more than 95% of all ectopic pregnancies occur in the fallopian tubes. Other sites include the ovaries, the abdominal cavity, the junction of the fallopian tube and uterus, and the cervix.
source
At other sites, an ultrasound of the abdomen and pelvis is usually performed first, using an abdominal scanner or an intravaginal one. So-called 'transvaginal' ultrasound is preferred in many centres, because it can detect pregnancies earlier than a 'transabdominal' one.
source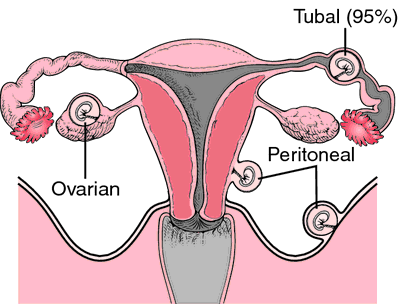 15) Where are your ovaries located in your body diagram?
15) Where are your ovaries located in your body diagram? This is one of the most asked questions in my referrers.
I have taught my daughter that if you make a triangle using your both hands, place the thumbs under your belly button, and your index fingers above your pubic bone, and everything in there is your reproductive system.

How to Locate your Reproductive Organs
The Uterus
Your uterus can be located by making an upside down triangle with your thumbs and index fingers. Join both your thumbs at your navel and extend your fingers downward, toward your pubic bone.
Your uterus is located where your fingers meet.
The Ovaries
Roughly measure four inches down from your navel and three inches to the right and left to locate your ovaries:
Go 4 inches (4 finger widths) below the navel. From this point, go 3 inches (3 finger widths) to the left and to the right.
source 16) What's a normal body temperature for a newborn?
16) What's a normal body temperature for a newborn? The normal body temperature for newborns is the same as adults, which can range between 98.6 to 99.5 degrees Fahrenheit or 36 to 37 degrees Celsius, according to the Mayo Clinic and the Birth website. A variation in normal body temperature, whether subnormal or elevated, can indicate the possibility of an infection, according to the Mayo Clinic.
source
If your newborn's temperature is slightly below the normal range, under 98.6 degrees Fahrenheit, he may need to be warmed up, according to the Birth website. Add additional layers of clothing or an extra blanket if necessary. If your newborn has a low-grade temperature, ranging in the upper 99 degrees Fahrenheit and just slightly below 100 degrees Fahrenheit, it does not register as a fever, according to the Birth website. Removing articles of clothing or blankets may help lower his temperature and no other treatment is required as long as he does not show other signs or symptoms of illness such as a cough or runny nose, according to the Birth website. Your newborn's temperature is considered a fever if his temperature reaches 100.4 to 101.3 degrees Fahrenheit, according to the Birth website. Fevers of this range may be due to a viral or bacterial infection. Newborn temperatures exceeding 101.3 degrees Fahrenheit warrant prompt medical attention.
source17) What to do with blighted ovum? Firstly, let's look at the term. Blighted Ovum sounds like something that goes wrong with mass corn production in agricultural areas in Iowa. But, sadly, it's not.
The term Blighted Ovum is a really crappy colloquial name for any anembryonic pregnancy. Simply, there's a shell for the pregnancy, an early form of placenta, but nothing is occupying the home. There is no baby nor will there ever be.
An anembryonic gestation (aka blighted ovum) is a pregnancy in which the very early pregnancy appears normal on an ultrasound scan, but as the pregnancy progresses a visible embryo never develops. In a normal pregnancy, an embryo would be visible on an ultrasound by six weeks after the woman's last menstrual period.
source 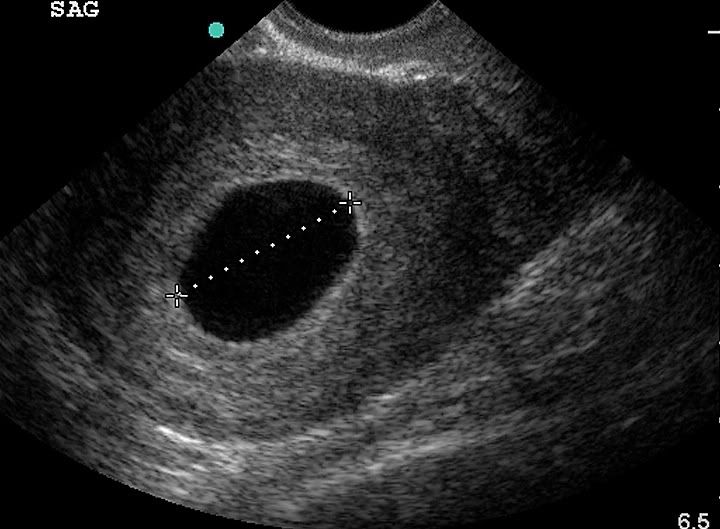
What you're looking at here is simply put: a shell of the pregnancy with nothing inside. There is no placenta forming.
A blighted ovum (empty gestational sac) occurs when a fertilized egg implants into the uterine wall, however, the fetus does not continue to develop past the sixth to eighth week of gestation. There is continued development of the placenta and amniotic sac which produces hCG (giving the positive pregnancy test).
sourceBasically, the genetic coding in the pregnancy has gone to the furtherest extent it could and simply corrupted. The body, acknowledging the hcg and respecting the process, has continued producing progesterone which gives the pregnant mother all the normal 1st trimester pregnancy symptoms.
However, the pregnancy cannot continue.
How common is a Blighted Ovum?
Approximate estimates indicate that 15% of all clinically recognized pregnancies end in miscarriage*. Estimates vary little and approximate blighted ovums account for 45 to 55% of all miscarriages**.
sourceHow is a Blighted Ovum confirmed?
During your scan, if the pregnancy sac measures more than 20mm, with no sign of an embryo, then your sonographer can make a diagnosis of a missed or silent miscarriage. The entire amniotic sac must be checked using vaginal ultrasound before the diagnosis can be confirmed. If the diameter is less than 20mm, the pregnancy may just be less advanced than you thought, and you will probably have another scan between seven and 14 days later. If there is still no sign of an embryo after this time, the diagnosis can be confirmed.
sourceWhat are the criteria for diagnosing a blighted ovum?
According to the Encyclopedia of Medical Imaging, the criteria for a diagnosis of blighted ovum are:
1) failure to identify an embryo in a gestational sac measuring at least 20 mm via transabdominal ultrasound.
2) Failure to identify an embryo in a gestational sac measuring approximately 18mm or more via transvaginal ultrasound.
3) Failure to identify a yolk sac in a gestational sac measuring 13mm or more.
Additionally, the outline of the sac may be irregular, incomplete or absent decidual reaction and/or fluid found in the gestational sac.
sourceWhat happens now?
This really is entirely up to you, the pregnant mother. A lot of women want confirmation it really is a pregnancy that will never end up with a live baby. And that is 100% fair and if you are feeling this way, please make it known.
A lot of doctors want to 'zap you in' for a D&C because they've seen it all before and know that it most likely is a blighted ovum and want you done and dusted.
However, you have the RIGHT to ask for up to a month for more repeated scans. The situation changes when you begin to bleed or have a fever. Then you must follow the orders of your doctor.
Like all failed pregnancies, the body must expel it as some point. A missed miscarriage is when the body fails to acknowledge the pregnancy has ended and continues to support it. The most common cause is a blighted ovum vs embryonic death.
The body must expel this pregnancy. It can take some time for the body to catch on, but a miscarriage is inevitable. The pregnancy will also begin to decompose at some stage and this is when you need to make sure you are receiving medical care as you do have the risk of becoming very ill.
My personal advice would be to wait 7 days and have a repeat blood hcg test and transvaginal scan. If there is no growth or appearance of a heartbeat, I would suggest you look to hurry the miscarriage process. Support group in forum format found at http://blightedovum.proboards46.com/
Support group in Yahoo email format found at http://health.groups.yahoo.com/group/blightedovumsupport/
18) What does the tissue mean when you have a miscarriage? Depending on the stage of your miscarriage, the length of the gestation and the amount of tissue you find, it can all mean different things.
Most tissue found when experiencing a first trimester miscarriage is your own tissue. By this I mean the endometrial lining that was supporting the pregnancy. It's basically the same as what you'd see during a heavy period.
Clotting is quite common in a miscarriage. Again, this is your own body's response to the miscarriage. The amount of blood is slightly more than you would experiencing in a period on your heaviest day.
If you are experiencing bleeding that is quite unusual to you, it's too fast, too heavy, too thick or full of tissue, you must, absolutely must, go to the Emergency Room/Emergency Department.
Most doctors would ask that you look at the miscarriage tissue to make sure you are not passing any sort of grape like blobs. They are quite apparent and suggest a molar pregnancy of some sort. You would know straight away if you had a molar pregnancy, because the tissue really does look and feel as though grapes were exiting your womb.
Molar Tissues
As for identifiable tissues: As for the appearance of miscarriage tissue, note that tissue from an early miscarriage may not be obvious to the naked eye. Many early miscarriages simply look like heavy menstrual periods, sometimes with tiny blood clots in the discharge.
If the miscarriage happened with development beyond four or five weeks gestational age, it is possible that there may be a small, transparent gestational sac with the rudimentary beginnings of a placenta on its edge.
If your miscarriage happened beyond six weeks, you may pass an identifiable embryo or fetus in the early stages of development, which may be as small as a pea or larger than an orange depending on how far along you were when the baby stopped growing. (Remember that it is a good idea to see a doctor if you are miscarrying, especially if you are in the later part of the first trimester or beyond).
Sometimes even in a later first-trimester miscarriage there may not be recognizable tissue, as sometimes the baby stops growing and begins to deteriorate before the onset of the miscarriage bleeding.
sourceIf you suspect you may be in your 2nd trimester, and you begin bleeding, go to the emergency department. A 2nd trimester miscarriage is a completely different experience to that of an early loss or 1st trimester miscarriage.
If you would like to see miscarriage tissue, follow this
link19) Was my miscarriage caused by drugs?This is a tricky question. Firstly, I am so sorry you are going through a miscarriage.
However, unless you are abusing recreational drugs, there really isn't much of an answer.
No, your miscarriage wasn't caused by taking antibiotics. Or Prozac. Or an antifungal cream.
Miscarriages happen because the genetic material simply ran out.
The pregnancy grew to the furtherest point it could before it simply stopped.
Antibiotics can't end a pregnancy. Nor can a beer before you know you're pregnant.
However, abusing drugs can. About 2 to 3% of all birth defects result from the use of drugs other than alcohol.
Smoking pot before you become pregnant can alter the chemicals in your own body. The egg you popped out might not have fully matured.
What do the drugs do?How a drug affects a fetus depends on the fetus's stage of development and the strength and dose of the drug. Certain drugs taken early in pregnancy (within 20 days after fertilization) may act in an all-or-nothing fashion, killing the fetus or not affecting it at all. During this early stage, the fetus is highly resistant to birth defects. However, the fetus is particularly vulnerable to birth defects between the 3rd and the 8th week after fertilization, when its organs are developing. Drugs reaching the fetus during this stage may have no effect, or they may cause a miscarriage, an obvious birth defect, or a permanent but subtle defect that is noticed later in life. Drugs taken after organ development is complete are unlikely to cause obvious birth defects, but they may alter the growth and function of normally formed organs and tissues.
sourceThe FDA has worked out a system for classifying drugs that may cause harm to an unborn child.
Category A drugs have shown no risk to the first trimester fetus of pregnant women, while Category B drugs have shown no risk in animal studies or have shown risk in animal studies but have shown no risk in human studies.
souceIt gets a bit grey when you get to C & D.
There have either been no studies conducted on drugs classified as Category C or D, or the studies show a risk but the benefits of the drug may outweigh the potential for harm.
souceIt is illegal to experiment on pregnant women. Therefore, the drug companies have to rely on submissions made by GPs and OBs to the company when an issue is found in a live birth. If your child died before birth, the GP or OB does not legally have to make a submission.
X
FDA-classified Category X drugs are harmful to the fetus and the benefits are not believed to ever outweigh the risks of miscarriage or birth defects; therefore these drugs should never be taken by pregnant women or those who plan to become pregnant.
souceWhich Drugs?
Most drugs classified under Category X that are associated with an increased risk of miscarriage are prescription only. These include the acne treatment isotretinoin, cholesterol-lowering drugs such as Lipitor, radioactive iodine, hormonal contraceptives including the morning-after pill, and the cancer treatment DES. Misoprostol and mifepristone are known to cause miscarriage and may be prescribed to either cause an abortion or to help an already occurring miscarriage along. Category D over-the-counter medicines may increase risks of birth defects or miscarriage and include aspirin and nicotine replacement therapies.
souceHerbs
Most people simply relate the term 'herb' to mean anything that grew from the ground up. Black pepper, paprika, oregano and basil are herbs. And harmless in usual amounts. And so things like ginseng, black cohosh and other herbs get marketed as safe and a lot of women reach for herbs during pregnancy because they assume they ARE safe.
They aren't.
When it comes to pregnancy, Herbs are drugs. A lot of conventional drugs are made from herbs. You must treat herbs with the same authority you treat little white tablets. Just because it has leaves and a flowering head doesn't marginalise it or make it safe.
Herbs including blue and black cohosh, basil root, and goldenseal may trigger uterine contractions, leading to miscarriage if you are not full term in the pregnancy. Other herbs such as ginseng and mugwort may cause birth defects.
souceIllicit drugs
Drugs taken by a pregnant woman reach the fetus primarily by crossing the placenta, the same route taken by oxygen and nutrients, which are needed for the fetus's growth and development. Drugs that a pregnant woman takes during pregnancy can affect the fetus in several ways:
*
They can act directly on the fetus, causing damage, abnormal development (leading to birth defects), or death.
*
They can alter the function of the placenta, usually by causing blood vessels to narrow (constrict) and thus reducing the supply of oxygen and nutrients to the fetus from the mother. Sometimes the result is a baby that is underweight and underdeveloped.
*
They can cause the muscles of the uterus to contract forcefully, indirectly injuring the fetus by reducing its blood supply or triggering preterm labor and delivery.
Some of the fetus's blood vessels are contained in tiny hairlike projections (villi) of the placenta that extend into the wall of the uterus. The mother's blood passes through the space surrounding the villi (intervillous space). Only a thin membrane (placental membrane) separates the mother's blood in the intervillous space from the fetus's blood in the villi. Drugs in the mother's blood can cross this membrane into blood vessels in the villi and pass through the umbilical cord to the fetus.
sourceIf you are using street drugs and you are pregnant, click over to
this resource and then contact your doctor or midwife. It's not healthy for YOU or your baby.
20) Vanishing twin ultrasound images/ Vanishing Twin SyndromeWhat is Vanishing Twin Syndrome?Vanishing Twin is another one of those odd colloquial terms doctors use in trying to explain what has happened in a pregnancy.
It's technical name is Intrauterine demise of a fetus in multiple pregnancies, ie. vanishing twin syndrome; vanishing triplet syndrome; vanishing quadruplet syndrome.
Vanishing twin syndrome was first recognized in 1945. Vanishing twin syndrome is when one of a set of twin/multiple fetuses disappears in the uterus during pregnancy. This is the result of a miscarriage of one twin/multiple. The fetal tissue is absorbed by the other twin/multiple, placenta or the mother. This gives the appearance of a “vanishing twin”.
souceThough it is blurry, this is one of the best Vanishing Twin ultrasounds I've seen.
It was captured at a time that shows positive growth of the live baby, but the arrested pregnancy still remains.

So, what is it anyways? * This concept was based on the findings that the incidence of early twin gestations was significantly higher than that noted later in pregnancy (about 5% versus 1 in 90 deliveries).
* Can occur at any time during the gestation but is most common in the first trimester.
* True loss rate is approximately 20% (1).
* Loss prior to 15 weeks gestation may result in no sonographic evidence of a twin pregnancy at a later date (pathologic examination at delivery may show no evidence that the twin ever existed) (2). This has been termed the "vanishing twin phenomenon" (1,3).
sourceWhat happens to the other twin?When a twin dies after the embryonic period of gestation, the water within the twin"s tissues, the amniotic fluid, as well as the placental tissue may be resorbed. This results in the flattening of the dead twin from the pressure of the growing twin2. Posner and Klein postulated that “the physical character of the dead fetus would appear to depend upon its position in the uterus with reference to the viable twin, the amount of amniotic fluid in each sac, the integrity of the chorion, and the time of death”3. The dead twin is described as either a “fetus compressus” or “fetus papyraceus”, depending on the degree of flattening.
With the advent of ultrasound, early loss of a member of a multiple gestation has been identified4,5 and has been described as “the vanishing twin”6 or the “vanishing twin syndrome”7. The vanishing rate has been reported as being as high as 71% of twin gestations diagnosed sonographically before the 10th week of gestation8. When twins were diagnosed between weeks 10 and 15, the loss rate was 63% in this same series. In the 79 patients whose multiple gestation was diagnosed after the 15th week of gestation, the loss rate was 0%. Robinson and Caines reported a similar loss rate of 53% when twin gestation was diagnosed in the first trimester9.
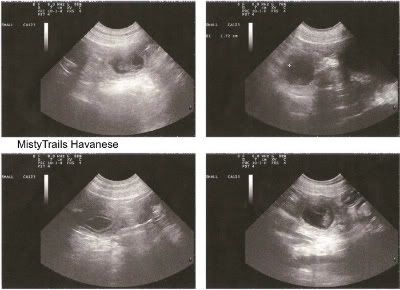
souce 21) Ultrasound pregnancy dogs
21) Ultrasound pregnancy dogsThis is an ultrasound of a dog who is currently pregnant.
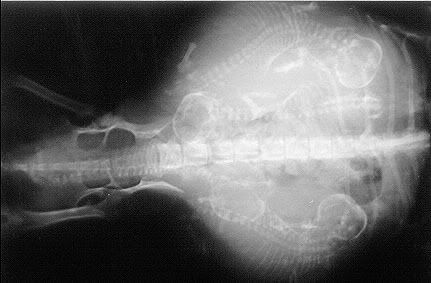
This is an xray of a dog who is currently pregnant.
 22) Should i get a medical bracelet for sulfa allergy?
22) Should i get a medical bracelet for sulfa allergy?
I think that's up to you. I have a sulfa allergy and have been administered a sulfa drugs TWICE despite both providers knowing my allergy.
I think if you are in a situation where you may become unconscious easily or frequently, then yes.
If you think you are in a situation where you can explain and relate your allergy to professionals, then no.
I need to get one.
23) Twin ConceptionEither the woman releases two eggs during her cycle rather than one (a process called hyperovulation) and each egg is fertilised by a different sperm, or the woman releases one egg which is fertilised in the normal way and subsequently splits in two. Twins in the former case are known as dizygotic or fraternal twins; in the latter, as monozygotic or identical twins.

Thus far, conceiving monozygotic (one-egg) twins is believed to be completely random, with no genetic component. The worldwide rate is constant at four births per thousand.
source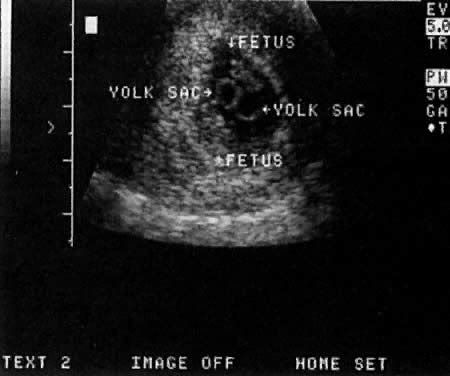 24) Sperm Meeting Egg
24) Sperm Meeting Egg A Visual Guide for All:
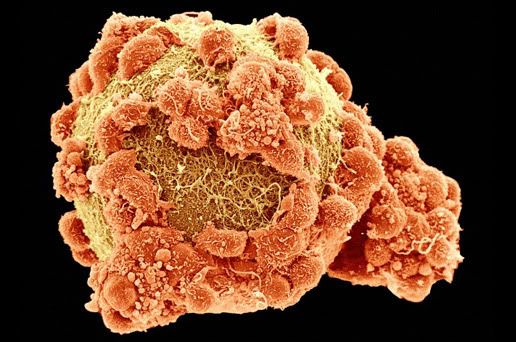
The Egg or OvaThis egg is still in the follicle and maturing.
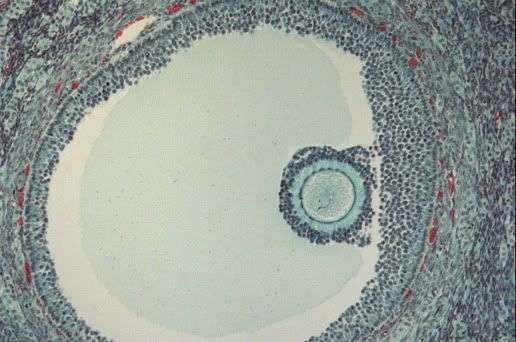
This egg is also still in the follicle and maturing.

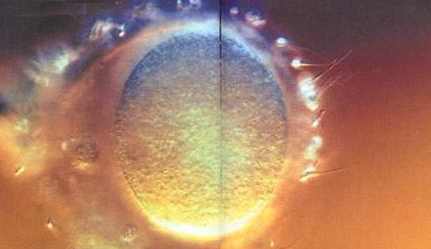
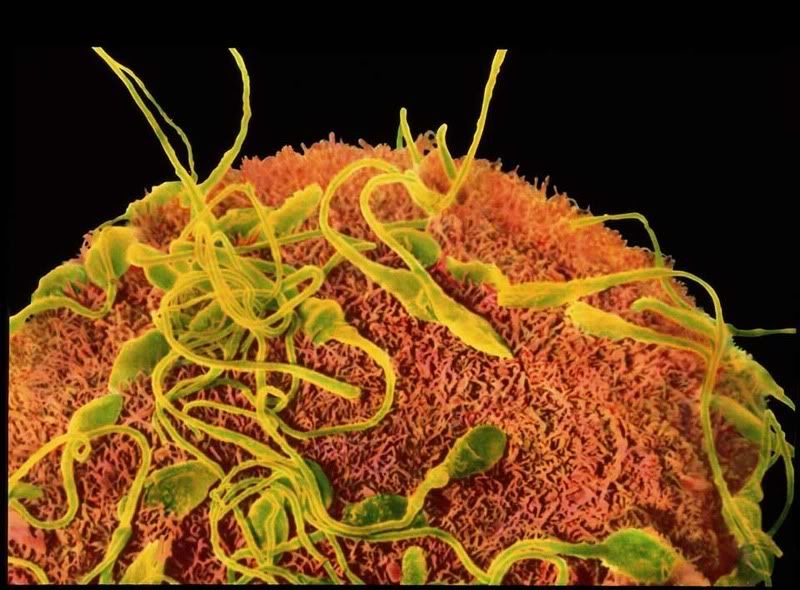
This ova has been released.
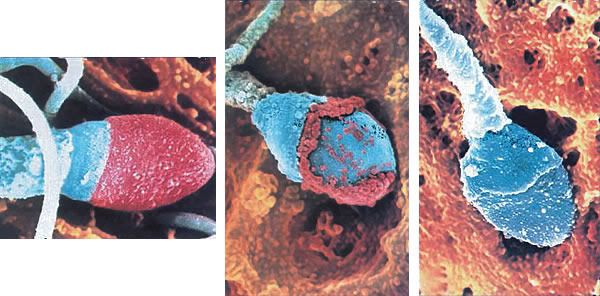
 The Sperm
The SpermThis image shows sperm (to the left) and tissue inside the testes (to the right).
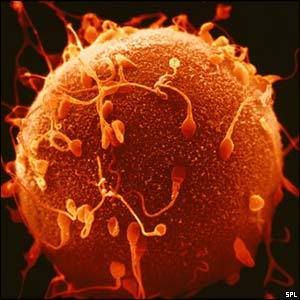
Sperm
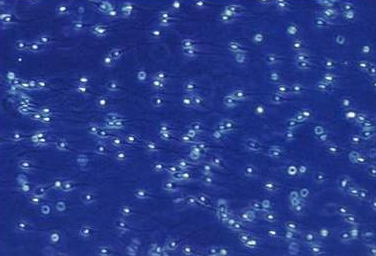
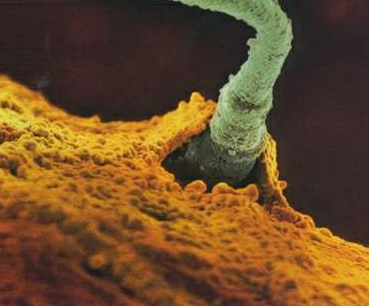
Sperm Meeting Egg or Boy Meets Girl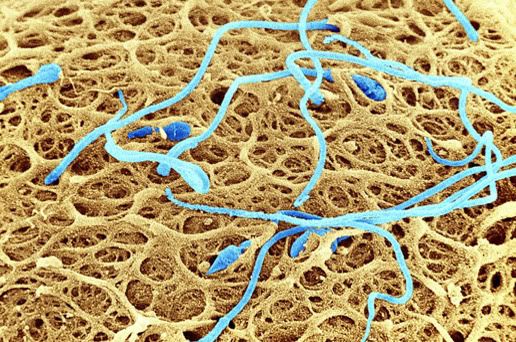

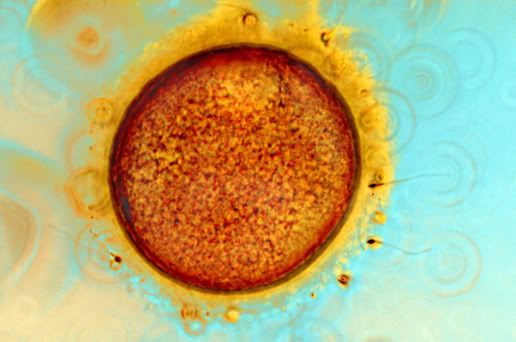



 And, 2 of the more common ways for Sperm to Meet Egg in the Hospital Setting:
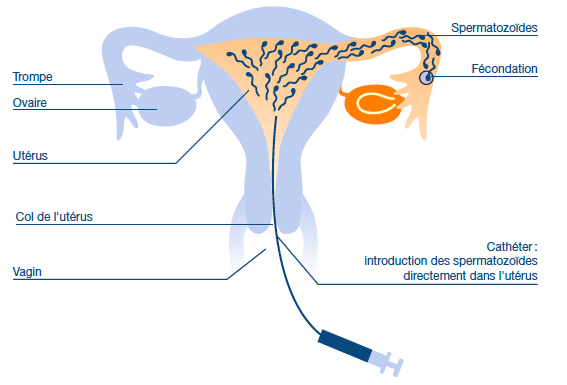
And, 2 of the more common ways for Sperm to Meet Egg in the Hospital Setting:IUI (Intrauterine Insemination)
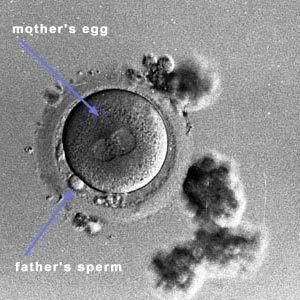
And, ICSI (Intracytoplasmic Sperm Injection)
 And what they all make:
And what they all make:
~~ L i f e ~~