

No One Expects to Miscarry
I was 21 when I had my first miscarriage. I was hugely surprised to be pregnant and was just as surprised when I miscarried. No one expects to miscarry.
After your first miscarriage, you begin to worry you will miscarry again. And, when you are predisposed to miscarriage, you suspect you will miscarry, and while you fervently pray it won't happen, you never expect it. You can sense it coming, but it is impossible to predict.
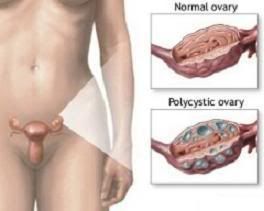
I have experienced miscarriage, and my predisposition is either from PCOS or because of the auto-inflammatory nature of Traps. It's taken me since May to put this together, so I hope it helps someone out there turning to Google for answers.
How often does pregnancy loss occur?
A woman's chance of miscarriage increases with her age. With increasing age, it not only becomes more difficult for a woman to get pregnant but to stay pregnant as outlined below:
In women ages 15 to 35, the incidence of miscarriage is between 10% and 12%.
In women ages 35 to 39, the incidence of miscarriage is 18%.
In women ages 40 to 44, the incidence of miscarriage is 33%.
In women ages 45-plus, the incidence of miscarriage is greater than 50%. -- source
Miscarriage is painful. I think it is more physically painful in the beginning and emotionally painful in the long-term. I also don't believe it is something that you get 'over'; you just get further from the pain with every dawning day.
When you have a threatened miscarriage (some still call it a threatened abortion), you can google and yet, as much as you can read and interpret, you can never prepare. Will it happen? When will it happen? Is there anything on earth I can do to stop it from happening? Is this considered spotting? Who named such a thing SPOTTING?! Did I do something to cause this? And then finally...
I remember posting on an Ivillage message board that I was miscarrying. The general response was that it was either 'the will of G-d' or 'a fortunate accident' because I was, after all, only 21. Having been told, at the age of 13, that I very likely had severe endometriosis, and a mother who refused to let them do a laparoscopy, I was glad to have been pregnant.
(I later had my laparoscopy in August 2003, was diagnosed with PCOS and uterine adhesions.)
Back then I had no idea what was going to happen. All I knew was that I had started bleeding lightly and the Internet told me I was having a miscarriage. And while this was an unplanned pregnancy, this was also an unplanned un-pregnancy.
Types of Miscarriage
Firstly, remember that a loss is a loss. A miscarriage is a horrible event that happens to good people and bad people, from the most deserving to least respectable. You cannot bring on a miscarriage by wishing you weren't pregnant just as you cannot desperately save a failing pregnancy with Hope alone.
However, it's often helpful to know terms that you may hear doctors or others bring up.

Chemical pregnancy -- "A chemical pregnancy occurs when an egg is fertilized but fails to develop successfully or implant fully in the uterus. A woman may miss her period and suspect she is pregnant; she may even have a positive pregnancy test because her body has produced some low—but detectable—levels of the pregnancy hormone hCG, but in a chemical pregnancy, there will be no gestational sac or placenta on ultrasound examination." -- source
Blighted ovum -- "A blighted ovum (or anembryonic pregnancy) refers to a fertilized egg that attaches to the wall of the uterus, begins to develop a placenta (which produces hCG), but then fails to develop into an embryo). What is left behind is an empty gestational sac (which can be visualized on an ultrasound)." -- source

Missed miscarriage -- "A missed miscarriage is when the embryo or fetus dies but continues to stay in the uterus. Often, the only signs of a missed miscarriage are the loss of all pregnancy symptoms, and less commonly, a brownish discharge. Confirmation of the miscarriage occurs when an ultrasound shows no fetal heartbeat." -- source

Incomplete miscarriage -- "An incomplete miscarriage is when some of the tissue from the placenta stays inside the uterus and some is passed through the vagina via bleeding. With an incomplete miscarriage, a woman continues to cramp and bleed (sometimes heavily), her cervix remains dilated, pregnancy tests still come back positive (or blood hCG levels are still detectable and don’t fall as expected), and parts of the pregnancy are still visible on an ultrasound." -- source

Threatened miscarriage -- "When there is some vaginal bleeding but the cervix remains closed and the fetal heartbeat (as seen on ultrasound) is still detectable, it is considered a threatened miscarriage. Roughly half of those women with a threatened miscarriage go on to have a perfectly healthy pregnancy." -- source
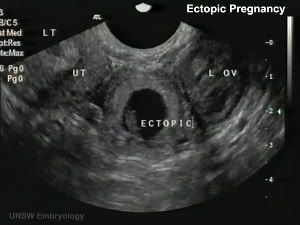
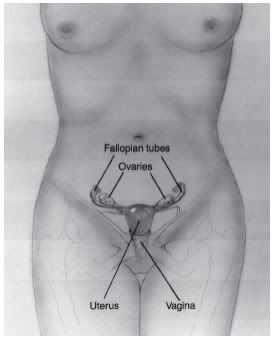
Ectopic Pregnancy -- "In a normal pregnancy, a fertilized egg travels through a fallopian tube to the uterus. The egg attaches in the uterus and starts to grow. But in an ectopic pregnancy, the fertilized egg attaches (or implants) someplace other than the uterus, most often in the fallopian tube. (This is why it is sometimes called a tubal pregnancy.) In rare cases, the egg implants in an ovary, the cervix, or the belly." -- source
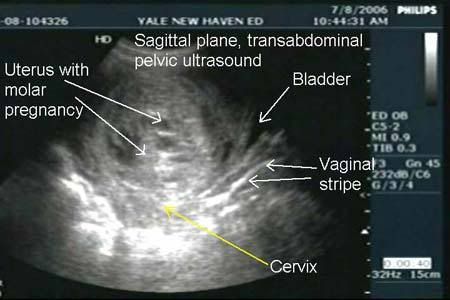
Molar Pregnancy -- "A molar pregnancy is a rare complication. It happens when an egg and a sperm meet at fertilization, but the cells do not grow in a way that can support a pregnancy. In a normal pregnancy, the fertilized egg has 23 chromosomes from the mother and 23 from the father, making a total of 46. In a molar pregnancy the wrong number of chromosomes come together, and there are abnormalities in the cells that grow to form the placenta." -- source
Terminal Prenatal Diagnosis -- "Before a baby would pass away and the family may not know what’s going on. Now potentially someone could have an abnormal screening and diagnosis at 12 weeks and have this whole pregnancy stretch ahead,” says Cheri Shoonveld, a genetic counselor for Fairview Health Services in Minnesota and a spokesperson for the National Society of Genetic Counselors. “Families are having to make a lot more decisions and have a lot more time to think about the impact." As a lot of these pregnancies end before the 20th week, most are classified as miscarriages. -- source
Recurrent Pregnancy Loss -- "Habitual abortion, recurrent miscarriage or recurrent pregnancy loss (RPL) is the occurrence of three or more pregnancies that end in miscarriage of the fetus, usually before 20 weeks of gestation. RPL affects about 0.34%[1] of women who conceive." The first time I heard a doctor use the term 'habitual abortion, I felt it was such a horrid term. It still gets to me.
"Recurrent pregnancy loss is a profound personal tragedy to the couples seeking parenthood and a formidably clinical challenge to their physician. While spontaneous abortion in approximately 15% of clinically diagnosed pregnancies of reproductive aged women, recurrent pregnancy loss occurs in about 1-2% of this same population." -- Marcelle Cedars, Marcelle I. Cedars, Infertility: practical pathways in obstetrics & gynecology. p 467.

Vanishing Twin Syndome -- "Vanishing twin syndrome was first recognized in 1945. Vanishing twin syndrome is when one of a set of twin/multiple fetuses disappears in the uterus during pregnancy. This is the result of a miscarriage of one twin/multiple. The fetal tissue is absorbed by the other twin/multiple, placenta or the mother. This gives the appearance of a “vanishing twin”." -- source

In the years that followed, more accurate details of miscarriage appeared online for the general audience and slowly more recognition of the pain of miscarriage and of honouring lost babies appeared. Today, loss mothers can reach one another at their moment of need and feel support. In 2002, it was very different.
Being at university, I crept into the library and looked for textbooks that might give me an idea of what was going to happen, but miscarriage wasn't covered in the basic anatomy books and as no one studied medicine at my uni, those books weren't abundant.

The staining was very light in the beginning, a floral pink. And the cramping was slow to start but became intense. I was pretty used to pelvic pain, what with the adhesions, but this was different. I started to feel nauseated and sweaty. I broke a sweat and felt the pangs of contractions, not knowing what they were.
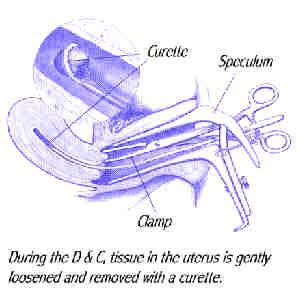
Over a period of a few hours, my cervix dilated and I began to bleed heavily, passing a maroon tissue, not dissimilar to raw chicken thighs, and saw swirls of light before my eyes. No one mentioned that in order to miscarry, one must give birth.
A Birth of a Different Kind
The cervix must dilate, not to the extremes of childbirth, but to allow the tissue and fetus to be expelled. The cervix then closes up and continues to bleed, much like a normal menstrual cycle, albeit heavier.
For most women, this is their first experience of birth and it can be frightening. Waves of contractions, nausea, sweats -- it seems like you're going crazy having to submit to this process that you don't even want, or may not even be aware of at the time.
If you have heavy bleeds to begin with, this can be extremely fatiguing as you do lose more than your normal amount of blood and it can seem like a whole lot at the time. The normal warning is that if you're going through more than 2 pads an hour, you need to go see the ER. Incomplete passage of tissue is very common and that can extend the amount of bleeding and pain as the cervix is still contracting to get it out and you're passing more fluid to try and free the tissue.
The Art of Miscarriage
Most miscarriages happen in the first few weeks of pregnancy, and a woman may not even know she's pregnant. I have pretty much always known because I become so unwell during those first few weeks. Sore boobs, headaches, nose bleeds, oh, and the puking. And the exhaustion. I think once you've experienced progesterone induced symptoms, you're more likely to recognize it the next time.
I generally get a sense of being 'less' pregnant right before a miscarriage. The nausea might drop off, the cramping ramps up and the exhaustion isn't so bad. I'm sure some women get varying degrees of pregnancy symptoms all through those first few weeks, but because I miscarry early, losing those symptoms seems to correspond with miscarriage for me. It seems to correspond with a distinct drop in progesterone and the drop in symptoms.
The only time the symptoms carried on was with my incomplete miscarriage before Sophie was born. I bled for weeks and passed little bits of tissue. I was just about to ask for a D&C to clear it all out when I realised it had stopped. I conceived Sophie just a couple weeks after that.
I feel it gave everything a good clean-out to prepare for her. The loss was also a Clomid cycle, so perhaps I had more lining in response.
Some literature claims that you bleed first and cramp second but I have experienced both, so I tend to think it's pretty impossible to tell a woman exactly how a miscarriage will progress for her. If every snowflake is different, so is every pregnancy and every pregnancy loss.
Squatting it Out: A Return to Ancient Times
Most women actually experience their miscarriages over the toilet or on the bathroom floor. There is something very natural about squatting during miscarriage and rocking on your knees can help the contractions. I've never experienced natural childbirth other than miscarriage, but I imagine it's pretty close to this.

As people tend to advocate for active birth, so should you seek an active miscarriage. Holing up in bed with tons of pain killers is one option, but personally I like the squatting and it's easier to clean up. I've seen women claim to want to experience miscarriage sans medicine but I have never done so. It hurts, I'm losing my baby and I'm bloody -- if I want some advil, I'm gonna take some advil.

Some doctors will write you a script for codeine based pills in anticipation of a miscarriage, but as you can't actually anticipate a miscarriage, it's best to take them when you feel the cramping begins. It's going to take a bit of time to get into your blood stream and contractions hurt. Depending on how well versed your cervix is in the art of dilating and contracting, it could be a long process or a relatively straight forward one.

When you consider something that is this small and tiny is coming out, you wonder why there is so much pain and so much STUFF.

Cute, ain't he?
Stuff
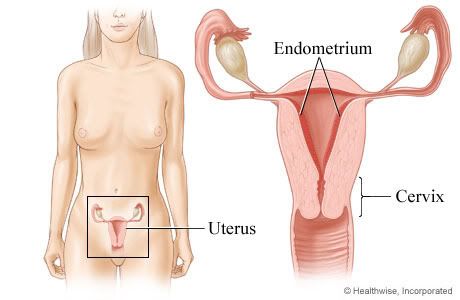
The truth is, there is a lot of stuff in there. Pre-placenta stuff, lining, embryo stuff, etc. And the cervix is a very delicate organ. It doesn't exactly enjoy your pap smears and being touched. So contractions really piss it off. No one likes an unhappy cervix, especially your cervix.
Some women tend to miscarry more in the late 2nd or 3rd month vs the very early miscarriages I have. I ovulate later, so I've been told my eggs aren't as 'good' as those who ovulate early or on time every cycle. I think it's rubbish, given that we ovulate when we're good and ready. Our bodies know a whole lot more than some stupid textbook or wheel.
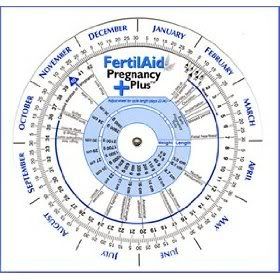
However, given the number of miscarriages I've had, well...maybe they are actually onto something with that wheel.
A larger fetus will accompany more STUFF that needs to be expelled. This is where doctors and nurses begin to worry about Incomplete Miscarriages. As someone who has had both a natural and surgical Incomplete Miscarriage, let me forewarn you about the completely minuscule chance of going septic. Because I did.
"Septicaemia is a recognised risk following miscarriage, as foetal material can be left behind in the womb acting as a reservoir for infection. In addition pregnant women have reduced immunity to allow them to carry the baby without rejecting it." -- source
It causes trouble, loads of it. And it can be prevented by having an ultrasound after you think you're finished miscarrying. Any doctor who refuses to do so isn't a doctor you want to keep company with. If you, like me, were stuck with just 1 at your disposal, badger, badger, badger until you get that scan.
It could very well save your life.
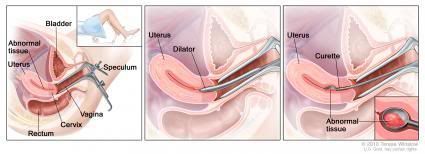
Management of Miscarriages
A fetus at this stage, 10 weeks, would most likely be a surgical miscarriage due to all the additional fluids, pieces and risks that could come with an incomplete miscarriage. However, it doesn't mean that you would *have* to opt for a surgical miscarriage.

If you did have a natural miscarriage at this stage, I would suggest that you need to have weekly blood draws to follow your hcg and a scan to make sure everything had passed. Often some placentas just don't unhinge the way they should and can remain.
The officially stop calling a miscarriage a miscarriage at 20 weeks. It then becomes a pre-term birth, a pre-term stillbirth or a stillbirth, which is something that is welcomed. In recent years, it was only considered a pre-term birth after 24 weeks. This has allowed so many more women the option of a birth certificate and burial for their baby. However, most women will never receive a birth certificate for their pregnancy loss, as these rules vary depending on local legislature.
I, personally, wish it was offered at any gestation, regardless of whether an insurance company or hospital director feels your baby was 'a cluster of cells', a 'product of conception' or not.
If you would like to order a stillbirth certificate for your own purposes, try these keepsake certificates.
Most women who miscarry after 12 weeks will need some form of medical management. Either the loss is very sudden and can involve hemorrhage or the labour will have to be induced. I have read internet accounts of women managing to use herbs to induce a labour and birth of their stillborn 14/15 week old baby, but if it were your first miscarriage, I don't think it would be very wise to attempt.
Some OBs recommend only having a D&E vs the induction of labour and birth at this stage. A later loss generally results in the induction of labour vs the surgical route. You will often find advice labeled "stillbirth treatment" vs induction of labour for stillbirth.
It is your right to ask for time to consider what will happen, unless you are in the middle of hemorrhaging or have a fever and are at risk of being septic. For some women, the idea of their child not being born into this world whole is a very tough one. They want to see, feel and hold their baby. And that should be their right, but, if the situation, your insurance, or your OB cannot allow that, you must, absolutely must, find a way of connecting to your baby after the D&E.
If you are having a miscarriage at an earlier gestation, you may find the doctor wants to quickly zap you into the OR and 'get it done'. Again, you have the choice unless it is medically unwise to do so. Take a day or two to think about it. Recurrent D&Cs have been known to cause scar tissue, but they most likely will not render you infertile no matter the quantity. It is the quality of the D&C and how gentle or firm the surgeon is at the time.
This is why you want someone skilled and NOT a medical student. No offense to medical students, but I will not be letting a junior surgeon near my womb ever again.
After Care
The length of gestation generally predicts the length of post-miscarriage bleeding, unless it was medically managed, and then it relies on how much of a hard hand the surgeon had. Post-miscarriage bleeding is healthy for the womb. It can go dark and represent old blood coming out and you can spot intermittently for weeks. If you've had a scan to give you the all clear and you're still spotting, it's probably just the womb recouping.
If you haven't had a scan and you're spotting, ask for one. And if you find that you begin to bleed again when exercising, doing housework or with an increase in exertion, see your doctor. That is a tell-tale sign of retained tissue.

They advise you not to have a bath or go swimming until you have stopped bleeding. I've read accounts of women swimming in the ocean after miscarriage and found it fine. I think the concern is inserting tampons, and possibly introducing bacteria in an already super sensitive organ. It needs to rest and no matter HOW much you hate pads, just don't go the tampon route. Let the womb heal as it needs.
Most women I've talked to have noticed the pains stop pretty much once the tissue has passed, but there may be some tenderness remaining, especially if you had a D&C or a D&E. If you have ongoing tenderness or an area that is sore to touch, you need to see a doctor. Again, risk of retained tissue or even a cyst on an ovary may be causing it.
Asking for the Tissues
If you had a medically managed miscarriage, it is 100% fine to ask for the tissues. You must make the surgeon aware and he/she must make the lab aware. Often they will want to take samples to test for chromosomal abnormalities but they do not need all of the tissue to do so. They often take quite a bit as some of the tissue will be your uterine lining and will test only as you, so they test quite a few pieces to make sure they get the baby's tissue.
Sometimes, and it's horrible when it happens, the tissue is lost, destroyed or denied a return to you.
I had my last D&C of my twin loss during a lab strike and the tissue was mismanaged and we never had it returned to us. Knowing it was the last chance I had to bury my twin girls and then never having them in a tangible way really got to me. How could someone just chuck my flesh and blood in a bin?
Sadly, it happens.
Coming to Grief

Lots of rest and feeling the emotions as they come are the best ways of coping in the days after a miscarriage. No matter what anyone says, you've just given birth to your baby, lost your baby and had to get up and carry on in a world that doesn't allow anyone to be less than normal.
Grief is an inevitable, ongoing process. It's a 24 hour a day, 7 day a week process. It is consuming and exhausting. And while it would be nice for us to have the time to focus solely on our grief, time passes, life goes on and our grief becomes a passive process.
It's good to make the time to take an active part in your grief. Craft plays a large part in dragging the passive into the active. Knitting. Gluing. Sewing. Stitching. Painting. Clay. Gardening. Hands moving without conscious thought. The mind drifts while the body work. Some find this release in sports. As long as whatever it is is a healthy choice, not obsessive, it's all good.
Grief is very different for men and women going through the same experience. It can be hard for a man to understand what is going on in your heart, in your mind. And you may find you do not know quite how to address your husband or partner's grief. Women in a lesbian relationship may find it hard to address the grief of the other because the experience is so different between partners.
You may be actively grieving while your partner is in a passive place. Or you might be stuck in a passive cycle and can't deal with the active grief of your partner.

Surviving Emotionally can be a very trying experience, especially if you have a demanding job or children at home. We all expect to come to grief at some stage in our lives, yes it is not something that is taught. Learning about grief, your emotions and learning about strategies to help you cope is all really preferable to letting the grief overwhelm you, passively, for months on end.
For some women, miscarriage can be a traumatic event which replays endlessly for them. If the loss was sudden or involved hemorrhage, post traumatic stress disorder or similar symptoms can develop as the woman struggles with the loss of control and the resulting loss of pregnancy. The emotional distress and anxiety can become encompassing. Depression following a traumatic miscarriage or a medically managed miscarriage is very common. Ongoing depression is often found in women who are undergoing infertility treatment who miscarry.

Take time. Today is not the day to decide if you're going to move onto IVF. Or whether you can afford IVF. Today isn't the day to start screening REs or question how many miscarriages they think you *need* to go through to get the recurrent miscarrier label.
Today is the day to mourn the loss of your dreams. Cry. Scream. Sing songs. Listen to the radio or cds. If you purchased things for your baby, you may feel the need to touch them or conversely, you may feel the need to pack them away. Please don't throw them all away today. Just fold it all up and put it somewhere else.
Feel what you are feeling. Denying these feelings is a recipe for disaster. If you are having a traumatic miscarriage, look into Post-traumatic Stress Syndrome. A lot of women who hemorrhage go on to develop a depression about what happened and how scary it was and how out of control they were. A ruptured ectopic can result in a similar experience in the loss of control, loss of blood and sudden loss of pregnancy.
Talk. To a counselor, a compassionate friend, pastor or relative. Don't entertain the company of people who tell you how you SHOULD be feeling or that what you're feeling is anything but normal, natural or useful. You are in mourning and you deserve the right to mourn safely however it suits you. Look into Elisabeth Kübler-Ross and seek to feel grief.
If you are a friend, partner, family member or relative of a woman going through pregnancy loss, please bookmark and save this resource from Baby Loss Comfort. There are things we desperately NEED you to say to us to open the conversation about our loss. Carly Marie Project Heal has a lovely page on what you CAN do to help those you love.
There are a lot of blogs, message boards and sites on the internet for loss mothers. Some are religious. Some are spiritual. Some are supportive and a few are troll-dens of childless women who want nothing more than delight in your pain. Avoid those ones. But open your willingness to become 'friends' with these women and share stories. And pictures.
I want to point you in the direction of Glow in the Woods. This is a fantastic first destination in opening the wound and inspecting and respecting your loss. The grief resources are also very good on this site.
Other loss mothers know how beautiful your precious baby is and how precious those photos are. If you are like most miscarriage mothers, you don't have a photo of your baby. I like to look at fetal photos of the same gestation and think about how he or she would have looked. Other loss mums get that.

Now is not the time to fall for 'get pregnant and never have another miscarriage' books, websites, vitamins, diets and whatever else people are boasting about on the internet. Certainly don't whip your credit card out to pay for these things. You may never have another miscarriage. You may have another. Right now is not the time to try and stitch together a plan that involves people preying on your pain.
If you need to actively purchase things, consider books on grief or baby loss, NOT trying to conceive or prevent miscarriage books. That time will come later. But for now, you need to delve into the grief and truly grieve. The beauty of books on loss and grief is that once you are done with them, you can donate them so that other mothers and fathers can read them too. Here is a good listing of titles to consider.
Remembering

Jizo is special to pregnant women and to those whose children have died. Statues of Jizo can sometimes be seen wearing tiny children's clothing or bibs. Grieving parents place toys and other offerings beside the Jizo statue to invoke his protection of their dead child. Offerings are also made by parents to thank Jizo for saving their children from a serious illness. -- source
When they tell you that it does get better, believe them but don't force the feelings to go away. It never truly stops hurting, but it stops hurting as much as it does today. There were days when I felt I'd never be able to take a deep breath because there were pins stuck in my lungs. Now, I feel guilty if I don't feel more sad on a daily basis.
Part of healing is remembrance. And part of remembering is grieving. Most of us don't have time to spend all day grieving, so our grief is a partial or obscured grief. When people look at you, they don't know the pain you're feeling. And you can't expect them too. You *can* expect to hear a lot of things that should never be uttered, but lots of people are working on education surrounding baby loss.
If you were able to obtain your baby's tissues, you can have a burial or cremation. Special boxes or bears have been designed to hold your baby's ashes.
If you haven't been able to request your baby's tissues, or like a lot of us, you never thought to save your baby's tissue (or it got flushed away in the toilet), remembrance jewelry is a good idea. This is also great for family and friends who want to support a grieving mother but can't think of an 'ok' gift for her.
La Belle Dame is a jewelry store that supplies memorial jewelry and has been supporting grieving families for a long time. They offer a key chain that can be given to the father or grandfathers.
If you are in Australia, you can order a Bear of Hope for families who are going through miscarriage and baby loss. Bears of Hope also do certificates of life for families in Australia as well.
Carly, at Christian's Beach takes photos of your baby's name at sunset, which can make for a beautiful reminder for the parents or grandparents.
I have not asked Carly for permission to put up one of her images yet, but I'm getting there. I hope she will say yes, because I want people experiencing loss to see her work. It is so shockingly, heart breakingly beautiful that you know it is from the heart of a loss mother.
For some of us, all we have is a name that never gets said yet lives on the tips of our tongue in anticipation of a moment we can speak it.
For me, it's Autumn and Isla. Born together, died together. Far too soon.
They were mine, and yet they weren't. You'd think I was crazy, but I live for a moment I can name them aloud. Pay tribute to their being. Pay tribute to their death. Pay tribute to the sadness, pain and grief in my heart.
I never even saw them, not even pieces of them. Swept away into a rubbish bin. Rotted. Decomposed, as if nothing could have ever come from them.
They would have been 4 this year. Big girls, at kindy. My darling twin babies.
A mother in mourning, I shall forever be.
If you, like me, are a Twin Loss mum (having lost one or both of your twins, at any stage, gestation or year, feel free to join us on Facebook at: Twin Loss NZ.
Yes, it's aimed at those of us living in NZ, but we welcome any mother who has had a twin loss. Twin Loss NZ has wonderful resources for any mother, especially aimed at those who have lost twins.
Life after Loss is difficult and the transition from Life Before Loss to Life After Loss is often fast, fragmented and fearful. But it is still Life. It is still worth living. Breath by Breath you can make it.

It isn't easy, but I promise it's worth it. <3

1 comments:
Just went through my first (and hopefully LAST) miscarriage. This post is amazing. Thank you!!
Post a Comment